The Oblique lumbar interbody fusion (OLIF) and Lateral lumbar interbody fusion (LLIF) also known as Extreme lateral interbody fusion (XLIF) or direct lateral interbody fusion (DLIF) are minimally invasive spinal procedures performed to treat back and leg pain caused by degenerative discs and other problems of the spine such as spinal stenosis, spondylolisthesis and spinal deformity.
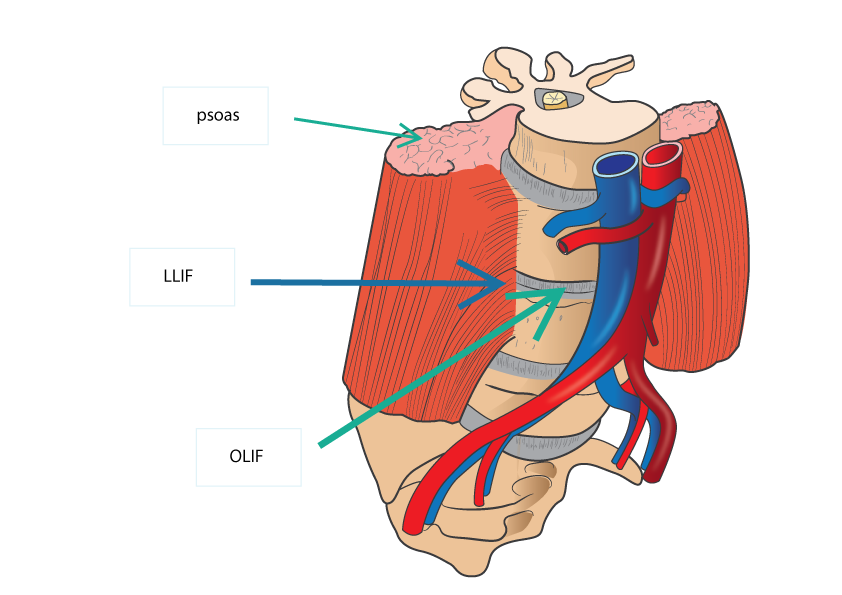
The Oblique lumbar interbody fusion (OLIF) utilised the plane between the vessels of the abdomen and psoas muscle (the muscles that helps flex the hip) while the Lateral lumbar interbody fusion (LLIF) involves seperating through the muscle of the psoas to reach the spine. Dr Lee can explain the pros and cons for either, but ultimately the choice is dependent on your anatomy.
There are a number of reasons why the OLIF or LLIF is advantageous over traditional posterior (back) approach, these include:
- Providing a more direct access to the disc to reconstruct a collapse disc space and deformity
- A larger cage can be used for reconstruction, which will allow better restoration of neural foramina (channels in which nerve exit the spinal column), improve stability and fusion rate
- Avoid going though scar tissue from previous spinal procedures from the back
- Avoid damaging muscles of the back Dr Lee can discuss this in detail with you should OLIF or LLIF is recommended for your condition.
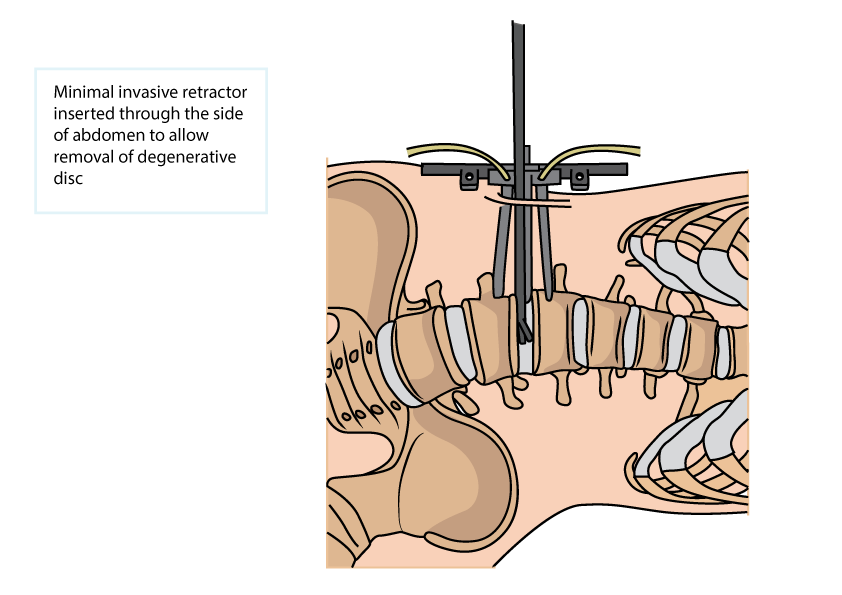
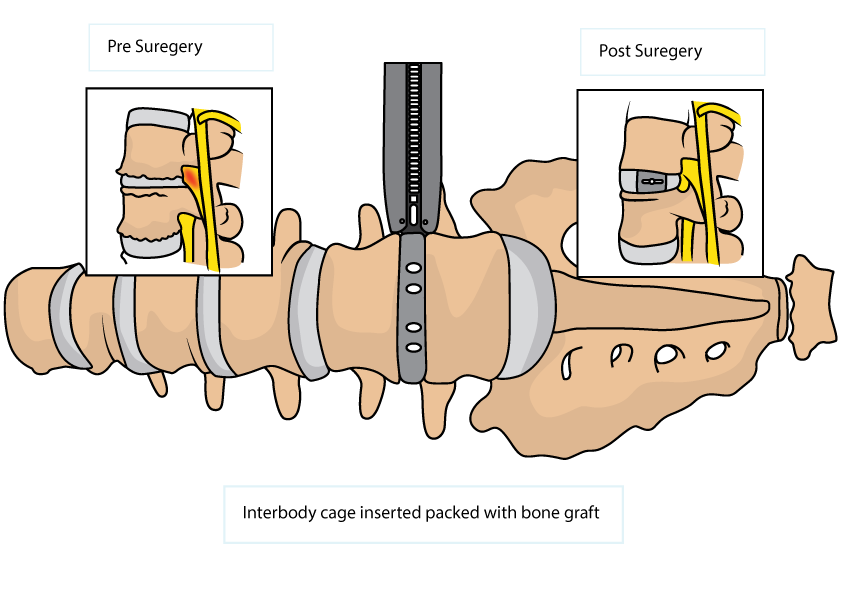
The procedures are performed under general anaesthesia. The patient is positioned on their side for surgery. The contents of the abdomen are moved to the side and the blood vessels are safely protected and the spinal disc is exposed. The psoas muscle which runs on the side of the spine is gently moved out of the way in OLIF and a minimally invasive spinal retractor is placed. For LLIF, or the XLIF or DLIF, the psoas muscle fibers are separated without dividing them. The disc is then removed and the spinal nerves are free off compression. The disc space is then measured and an appropriate sized cage is selected. This is then filled with bone graft, and then this is placed into the empty disc space. Occasionally a plate and screws are also placed at this time to further enhance the stability of the construct. The retractors are then removed and the incision is closed.
In some patients, additional approach through the back may be required to decompress the nerves. Screws and rods may need to be inserted above and below the disc space to aid stability while the fusion takes place. Dr Lee commonly inserts these screws through minimally invasive techniques.
Dr Lee can discuss this in detail with you should OLIF or LLIF be recommended for your condition.